Cancer Difficulty & Survival Estimator
Select Cancer Type
Diagnosis Stage
See FAQ for details.
Select a type to begin
Select a cancer type and stage to view estimated survival rates and key biological challenges.
You hear the word "cancer" and your mind might race to statistics about breast or lung cancer. But when oncologists talk about the absolute toughest battles in modern medicine, they aren't talking about the most common ones. They are talking about tumors that hide well, resist drugs, and spread before anyone notices. If you are asking what is the hardest cancer to treat, you are looking for the diseases where early detection fails, standard therapies struggle, and survival rates remain stubbornly low despite decades of research.
The short answer isn't just one disease. It is a small group of aggressive malignancies that share specific traits: biological complexity, late-stage diagnosis, and resistance to chemotherapy. Today, we will break down why pancreatic cancer, glioblastoma, and certain types of lung cancer sit at the top of this difficult list. We will also look at why these cancers behave the way they do and what current medical science is doing to fight back.
Why Some Cancers Are Harder Than Others
Not all cancers are created equal. The difficulty of treating a cancer depends on three main factors: how fast it grows, where it is located, and how it reacts to treatment. Most cancers respond to some form of chemotherapy, radiation, or immunotherapy. The "hardest" cancers resist all three.
First, consider location. Tumors in organs like the brain or pancreas are physically shielded from many drugs. The blood-brain barrier, for example, is designed to keep toxins out of the brain, but it also blocks most chemotherapy drugs. Second, consider biology. Some cancer cells mutate rapidly, meaning a drug that works today might fail tomorrow because the tumor has evolved. Finally, consider detection. Many hard-to-treat cancers show no symptoms until they have already spread to other parts of the body. By the time a patient feels pain or loses weight, the window for curative surgery may have closed.
| Factor | Impact on Treatment | Example Cancers |
|---|---|---|
| Physical Location | Blocks drug delivery; limits surgical options | Glioblastoma, Pancreatic Cancer |
| Biological Aggressiveness | Rapid mutation leads to drug resistance | Small Cell Lung Cancer |
| Late Detection | Cancer spreads before symptoms appear | Pancreatic Cancer, Ovarian Cancer |
| Tumor Microenvironment | Creates a protective shield around tumor cells | Pancreatic Ductal Adenocarcinoma |
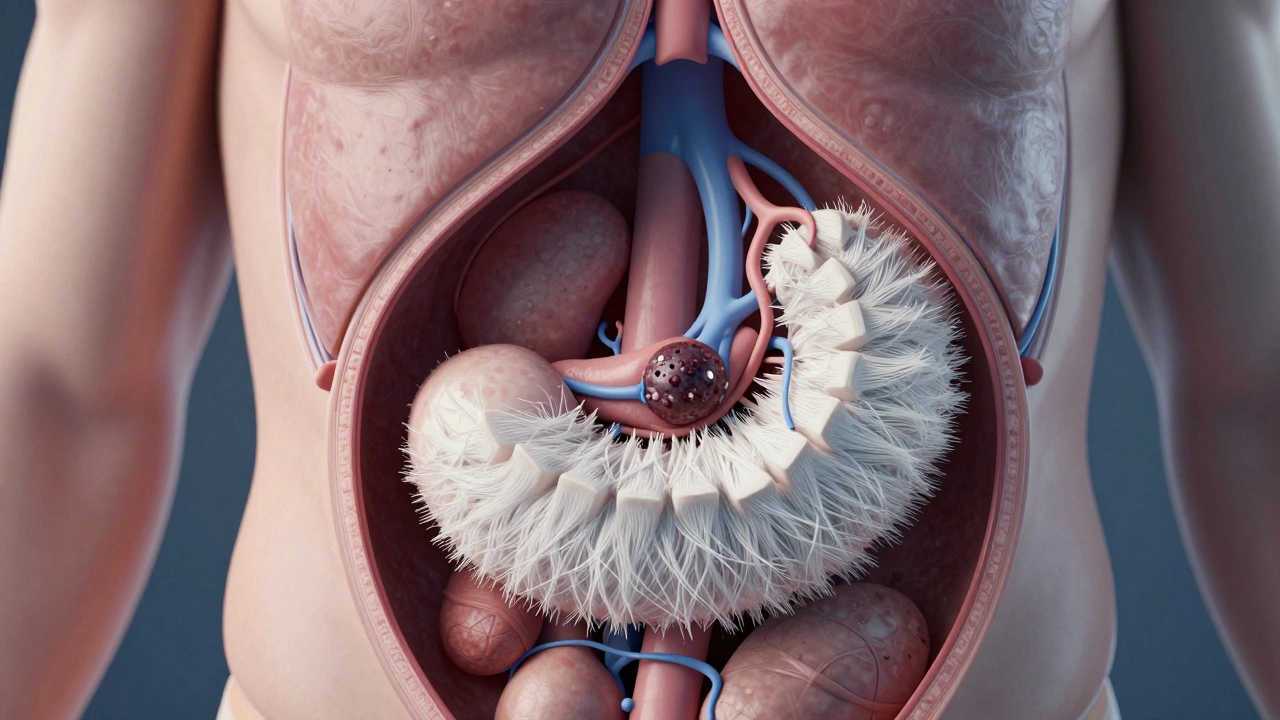
Pancreatic Cancer: The Silent Killer
If there is one cancer that consistently ranks as the most difficult to treat, it is Pancreatic Cancer, specifically Pancreatic Ductal Adenocarcinoma (PDAC). This type accounts for over 90% of pancreatic cases. It is often called the "silent killer" because the pancreas sits deep in the abdomen, behind the stomach. When a tumor grows here, it rarely causes pain or visible symptoms until it is large enough to press on nerves or block bile ducts.
By the time a patient visits a doctor with jaundice (yellowing of the skin) or unexplained weight loss, the cancer has often metastasized to the liver or lungs. Only about 15% of patients are diagnosed early enough for surgery, which is the only potential cure. For the remaining 85%, treatment focuses on extending life rather than curing the disease.
Even when surgery is possible, the biology of PDAC is hostile. These tumors are surrounded by a dense stroma-a thick layer of fibrous tissue that acts like a fortress. This stroma prevents chemotherapy drugs from penetrating the tumor effectively. Furthermore, pancreatic cancer cells are highly resistant to apoptosis, the natural process where damaged cells self-destruct. This means that even if a drug damages the DNA of a cancer cell, the cell often refuses to die.
Survival rates reflect this difficulty. According to data from the American Cancer Society, the five-year relative survival rate for localized pancreatic cancer is around 44%. However, for distant (metastatic) disease, the rate drops to approximately 3%. While new treatments like FOLFIRINOX chemotherapy regimens have improved outcomes slightly compared to older methods, the prognosis remains grim for most patients.
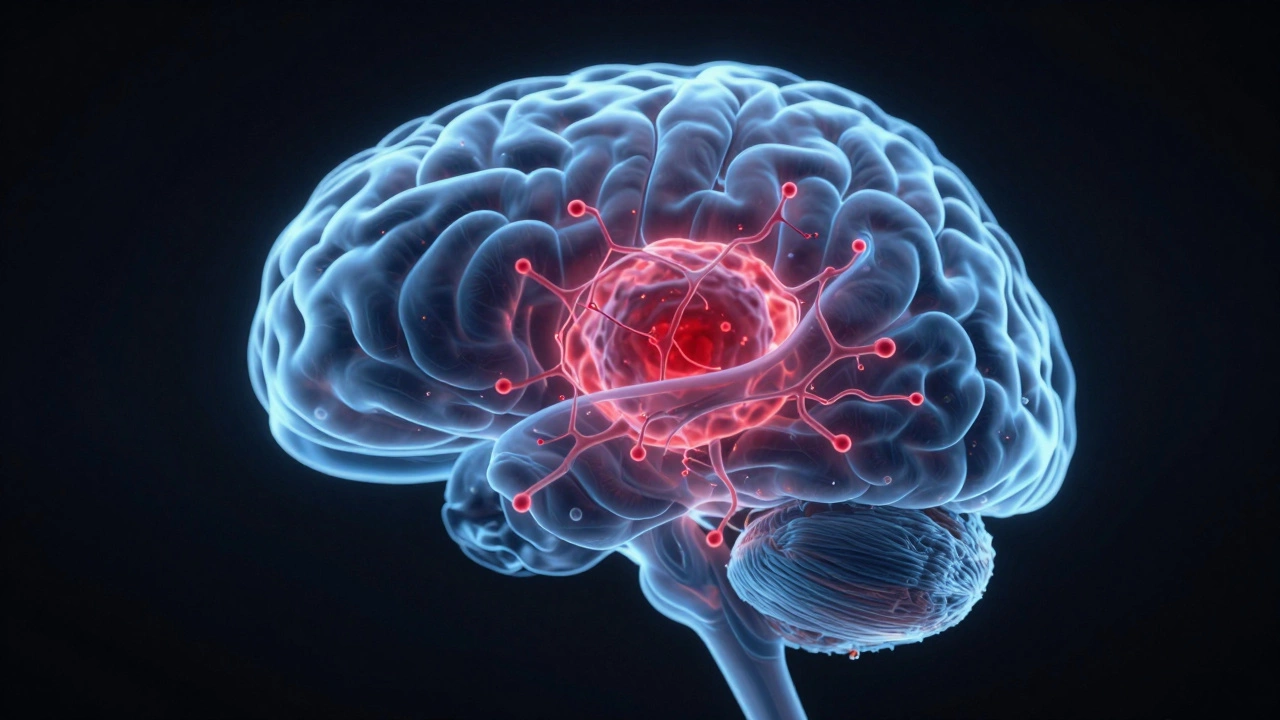
Glioblastoma: The Brain's Most Aggressive Tumor
Glioblastoma (also known as Glioblastoma Multiforme or GBM) is the most common and aggressive primary brain tumor in adults. Unlike pancreatic cancer, which hides in the abdomen, glioblastoma is hidden in plain sight within the brain, yet it is incredibly hard to reach and eradicate.
The primary challenge with glioblastoma is the blood-brain barrier. This protective membrane surrounds the brain and spinal cord, filtering out harmful substances. Unfortunately, it also filters out most conventional chemotherapy drugs. Doctors can use high-dose oral temozolomide, which can cross the barrier to some extent, but its effectiveness is limited. Radiation therapy is used, but because the tumor infiltrates healthy brain tissue, doctors cannot simply cut it all out without causing severe neurological damage.
Glioblastomas are also biologically chaotic. Within a single tumor, you can find different subtypes of cells, each with unique genetic mutations. This heterogeneity means that while a treatment might kill one type of cell, another type survives and continues to grow. Recurrence is almost inevitable. Even after successful surgery and aggressive post-operative therapy, the median survival time is typically between 12 and 18 months. Five-year survival rates hover around 6-7%.
Researchers are exploring new avenues, such as convection-enhanced delivery (CED), which involves surgically placing catheters directly into the tumor to deliver drugs locally, bypassing the blood-brain barrier. Immunotherapies and targeted therapies are also under investigation, but none have yet become a standard cure.
Small Cell Lung Cancer: Speed and Spread
When people think of lung cancer, they often imagine non-small cell lung cancer (NSCLC), which has seen significant advances in targeted therapies. However, Small Cell Lung Cancer (SCLC) is a different beast entirely. SCLC accounts for only about 13-15% of lung cancer cases, but it is far more aggressive.
SCLC is characterized by rapid growth and early spread. It usually starts in the center of the chest near the bronchi and quickly metastasizes to the brain, bones, liver, and adrenal glands. Because it grows so fast, patients often present with advanced disease. In fact, about two-thirds of patients are diagnosed with extensive-stage SCLC, meaning the cancer has spread beyond one side of the chest.
Initially, SCLC responds very well to chemotherapy and radiation. Patients often see their tumors shrink dramatically within weeks. This creates a false sense of security. However, the cancer cells quickly develop resistance to these drugs. Relapse is common, and once the cancer becomes refractory (stops responding to treatment), options are extremely limited. The five-year survival rate for extensive-stage SCLC is less than 3%.
Recent years have seen the introduction of immunotherapy drugs like atezolizumab and durvalumab in combination with chemotherapy, which has modestly improved survival times. Yet, the fundamental challenge remains: SCLC evolves faster than our current drugs can keep up.
Other Notable Challengers
While pancreatic cancer, glioblastoma, and small cell lung cancer are often cited as the hardest, other cancers pose significant challenges due to specific biological or diagnostic hurdles.
- Ovarian Cancer: Often called a "silent" disease, ovarian cancer typically presents vague symptoms like bloating or abdominal discomfort, leading to late diagnosis. About 75% of cases are diagnosed at an advanced stage. While initial chemotherapy often works, the cancer frequently returns and becomes resistant to platinum-based drugs over time.
- Hepatocellular Carcinoma (Liver Cancer): This cancer often develops in livers already damaged by cirrhosis or hepatitis. This limits treatment options because the liver cannot tolerate aggressive surgeries or high doses of chemotherapy. Targeted therapies and immunotherapies have helped, but survival rates remain low for advanced stages.
- Mesothelioma: Strongly linked to asbestos exposure, mesothelioma affects the lining of the lungs or abdomen. It has a long latency period (decades after exposure) and is often diagnosed at a late stage. Its location makes complete surgical removal nearly impossible.

Why Do These Cancers Resist Treatment?
Understanding why these cancers are so hard to treat requires looking at their cellular behavior. One key mechanism is drug efflux. Cancer cells can pump chemotherapy drugs out of themselves before the drugs can cause damage. Another is angiogenesis, where tumors create their own blood supply to fuel growth while isolating themselves from the immune system.
Furthermore, the concept of "tumor microenvironment" is crucial. In pancreatic cancer, for instance, the tumor recruits normal cells to build a protective scaffold. This environment suppresses the immune system, preventing T-cells from attacking the cancer. Immunotherapies, which have revolutionized treatment for melanoma and lung cancer, have struggled to work in these "cold" tumors where immune cells cannot penetrate or activate.
Hope on the Horizon: New Approaches
Despite the grim statistics, research is accelerating. Precision medicine is changing the landscape. Instead of treating "pancreatic cancer" as a single entity, doctors now test tumors for specific genetic mutations. For example, a small percentage of pancreatic cancer patients carry BRCA mutations. These patients may respond better to PARP inhibitors, a class of drugs that target DNA repair mechanisms.
In glioblastoma, clinical trials are testing vaccines that train the immune system to recognize tumor-specific antigens. For small cell lung cancer, researchers are investigating novel combinations of immunotherapy and targeted agents to delay resistance.
Artificial intelligence is also playing a role. AI algorithms are being trained to detect subtle signs of pancreatic cancer on CT scans years before symptoms appear. Early detection is the single most powerful tool against these aggressive cancers. If we can catch them earlier, even difficult cancers become manageable.
What Can Patients Do?
If you are concerned about risk factors, awareness is your first line of defense. Know your family history. Pancreatic cancer, for instance, runs in families with genetic syndromes like Lynch syndrome or BRCA mutations. If you have a strong family history, ask your doctor about screening protocols.
Avoid smoking. Smoking is the leading preventable cause of pancreatic cancer and is strongly linked to small cell lung cancer. Quitting at any age reduces risk significantly. Maintain a healthy weight and limit alcohol consumption, as these factors contribute to liver and pancreatic health.
Pay attention to your body. Unexplained weight loss, persistent abdominal pain, changes in bowel habits, or new neurological symptoms should never be ignored. While these symptoms can be caused by benign conditions, they warrant immediate medical investigation.
Is pancreatic cancer always fatal?
No, but it is often fatal if not caught early. When pancreatic cancer is detected at a localized stage (confined to the pancreas), the five-year survival rate is around 44%. However, most cases are found at later stages, where survival rates drop significantly. Surgery offers the best chance for a cure, but only a minority of patients are eligible.
Can glioblastoma be cured?
Currently, there is no cure for glioblastoma. It is considered a chronic, progressive disease in most cases. Standard treatment involves surgery to remove as much of the tumor as possible, followed by radiation and chemotherapy. While this can extend life and improve quality of life, the tumor almost always recurs. Research into new therapies is ongoing.
Why is small cell lung cancer so aggressive?
Small cell lung cancer (SCLC) grows and spreads faster than other types of lung cancer. It tends to metastasize early, often before symptoms appear. Additionally, while it initially responds well to chemotherapy, the cancer cells quickly develop resistance, leading to relapse. This rapid evolution makes long-term control difficult.
Are there genetic tests for pancreatic cancer risk?
Yes. Genetic testing can identify mutations in genes like BRCA1, BRCA2, PALB2, and CDKN2A, which increase the risk of pancreatic cancer. If you have a family history of pancreatic, breast, or ovarian cancer, discuss genetic counseling with your healthcare provider. High-risk individuals may benefit from regular screening with MRI and endoscopic ultrasound.
How does the blood-brain barrier affect cancer treatment?
The blood-brain barrier is a protective layer that prevents harmful substances from entering the brain. Unfortunately, it also blocks most chemotherapy drugs from reaching brain tumors like glioblastoma. This makes systemic treatment less effective. Researchers are developing methods to temporarily open the barrier or deliver drugs directly into the tumor via surgery.